지난 편에서 우리는 인류 최초의 펩타이드 약물이자 유전자 기술을 응용한 최초의 약물인 인슐린에 대해 살펴보았습니다. 이번 글에서는 우리 몸에서 자연스럽게 분비되는 이 중요한 호르몬, 인슐린과 함께 인슐린 저항성에 대해 좀 더 깊이 있게 이해하는 시간을 가질 겁니다.
대사증후군: 우리의 예상보다 가까이 있는 위험
최근 2024년 발표된 자료에 따르면, 대한민국 65세 이상 성인의 약 절반(47.0%)이 대사증후군을 겪고 있다고 합니다. 이는 비단 우리나라만의 문제가 아닙니다. 전 세계적으로 대사 건강 문제는 심각하며, 고령화와 함께 그 유병률은 더욱 높아지고 있습니다.
우리는 흔히 대사증후군을 이야기할 때 혈압, 혈당, 중성지방, 콜레스테롤, 복부 지방 등 개별적인 수치에 집중하곤 합니다. 하지만 이 모든 지표가 복합적으로 얽혀 나타나는 대사증후군은 단순한 개별 수치들의 합을 넘어섭니다. 이처럼 다양한 증상들이 한데 묶여 나타나는 현상 뒤에는 어떤 공통적인 원인이 숨어 있는 걸까요?
인슐린 저항성: 대사 문제의 핵심 열쇠
현대 의학은 20세기 초반부터, 특히 1960년대 이후 활발하게 진행된 연구를 통해 대사증후군과 수많은 만성 질환의 근본적인 원인 중 하나로 인슐린 저항성을 지목해 왔습니다.
의료 전문가들은 인슐린 저항성을 “우리 몸의 세포가 인슐린 호르몬에 정상적으로 반응하지 못하는 상태이며, 이로 인해 췌장이 과도하게 인슐린을 분비하는 고인슐린혈증이 발생한다”고 간단히 설명하기도 합니다. 하지만 때로는 너무 압축적인 정보가 오히려 핵심을 놓치게 만들 때도 있죠. 인슐린 저항성의 의미와 그 메커니즘을 좀 더 구체적으로 파고들어 볼 필요가 있습니다.
인슐린 저항성과 그 메커니즘
인슐린은 단순히 포도당을 세포로 “안내”하는 역할만 하는 것이 아닙니다. 인슐린은 세포가 포도당을 효과적으로 흡수하고 이용할 수 있도록 “지시”하는 신호 전달 물질로서의 역할을 수행합니다.
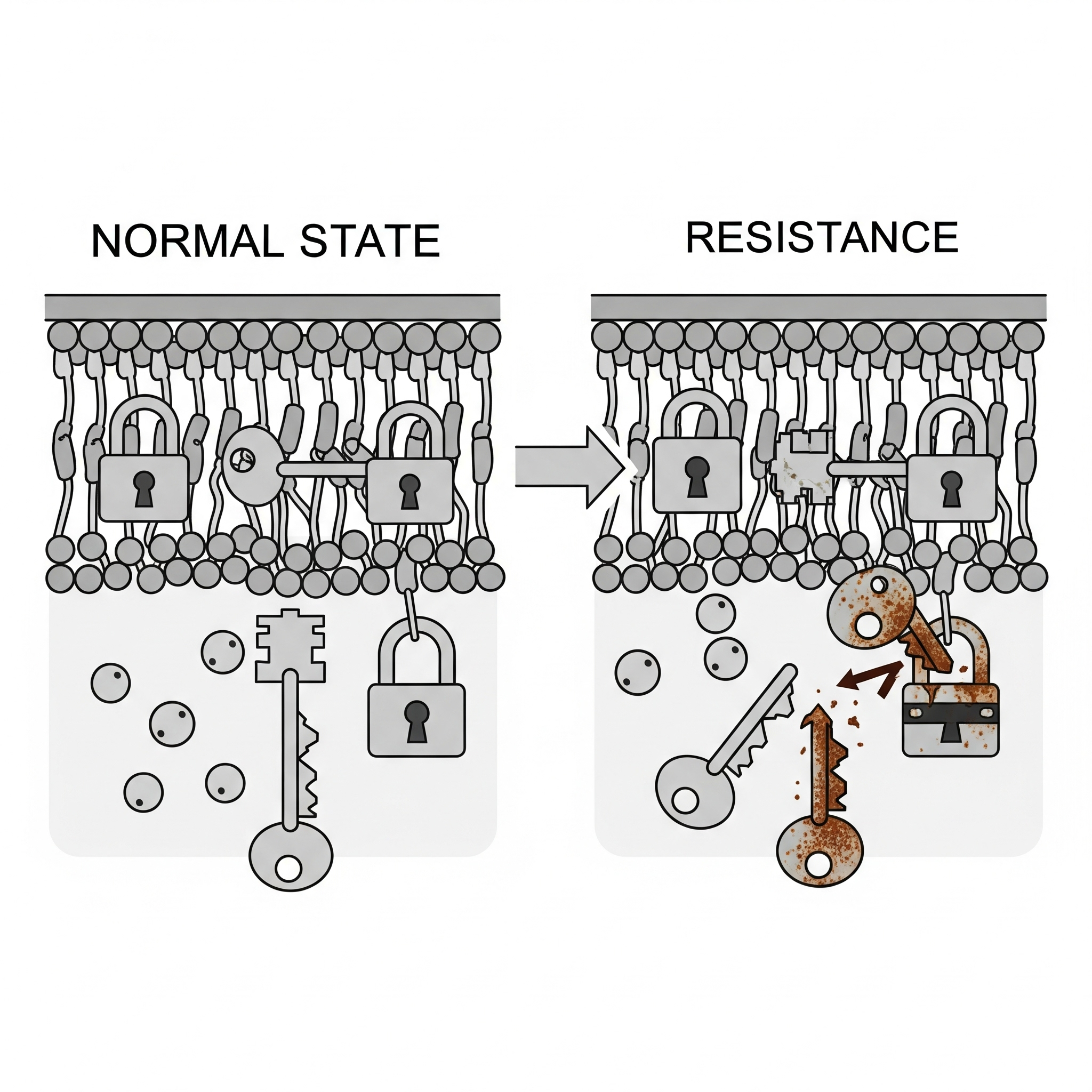
- 인슐린의 표적 조직과 수용체: 인슐린이 특정 세포에 작용하려면 해당 세포 표면에 인슐린 수용체가 있어야 합니다. 인슐린이 이 수용체에 결합하면 세포 내부로 일련의 신호가 전달되고, 이 신호에 따라 포도당 운반체가 세포막으로 이동하여 포도당이 세포 안으로 들어갈 수 있는 통로를 열어줍니다. 인슐린 저항성은 바로 이 수용체와 그 이후의 신호 전달 과정에 문제가 생겨 세포가 인슐린의 지시에 둔감해지는 것을 의미합니다.
- 포도당이 없는 장기: 우리 몸의 일부 장기(예: 뇌의 일부, 적혈구)는 인슐린의 도움 없이도 포도당을 흡수할 수 있는 특정 포도당 수용체(GLUT1, GLUT3 등)를 가지고 있습니다. 이러한 장기들은 인슐린 저항성의 직접적인 영향을 받지 않습니다. 그러나 인슐린 저항성의 주된 표적은 간, 골격근, 지방 조직이며, 이들 조직에서 인슐린 저항성이 발생하면 전신적인 혈당 조절에 심각한 문제가 초래됩니다.
인슐린의 지방 대사 관여: 단순히 혈당 문제가 아니다
인슐린은 단순히 포도당 대사뿐만 아니라 지방 대사에도 깊이 관여합니다.
- 지방 축적 촉진: 인슐린은 간과 지방 조직에서 지방산 합성을 촉진하고, 지방세포로 포도당을 흡수시켜 중성지방으로 전환하여 저장하는 핵심적인 역할을 합니다.
- 지방 분해 억제: 또한 지방세포에서 지방이 분해되는 것을 억제합니다. 즉, 인슐린은 우리 몸이 에너지를 저장하고 지방을 축적하는 데 매우 중요한 호르몬입니다.
인슐린 저항성 발생 시: 인슐린 저항성이 생기면 이러한 지방 대사 조절 기능에도 문제가 발생합니다. 지방세포가 인슐린 신호에 둔감해지면 혈중 지방산 수치가 높아지고, 이는 다시 간으로 가서 지방간을 유발하거나 다른 조직에 비정상적으로 지방이 축적되는 **이소성 지방(Ectopic Fat)**을 초래하게 됩니다. 그리고 이 이소성 지방은 다시 인슐린 저항성을 악화시키는 악순환을 만들어냅니다.
이처럼 인슐린 저항성은 단순히 혈당 조절 문제에 그치지 않고, 포도당과 지방 대사 전반에 걸친 복합적인 이상을 초래하며, 이것이 결국 대사증후군과 제2형 당뇨병, 심혈관 질환, 더 나아가 특정 유형의 암(유방암, 췌장암 등)의 원인이 될 수 있습니다.
Reaven(1988)과 DeFronzo & Ferrannini(1991)를 비롯한 여러 연구 결과들은 고인슐린혈증이 대사 이상과 대사증후군의 다양한 증상들을 야기하는 핵심적인 기전임을 보여주고 있습니다. 그리고 이 고인슐린혈증의 가장 근본적인 원인은 바로 음식물로 섭취하는 포도당 또는 포도당으로 쉽게 전환될 수 있는 소화성 탄수화물의 만성적인 과다 섭취에서 비롯됩니다.
참고 문헌
인슐린 저항성에 대한 이해는 수십 년간의 방대한 연구를 통해 발전해 왔습니다. 다음은 이 분야의 주요 이정표가 된 문헌들입니다.
- Himsworth, H. P. (1939). Diabetes Mellitus: Its Differentiation into Insulin-Sensitive and Insulin-Insensitive Types. The Lancet, 233(6022), 127-130.
- 간략한 내용: 인슐린이 발견된 지 얼마 되지 않은 시점(1921년)에 이미 당뇨병을 인슐린에 민감한 유형과 인슐린에 둔감한 유형으로 구분하려는 초기 시도를 보여주는 중요한 논문입니다. 이는 현대의 ‘인슐린 저항성’ 개념의 초석이 되었다고 볼 수 있으며, 인슐린에 대한 반응성 차이가 질병의 근간에 있을 수 있다는 통찰을 제시했습니다.
- Reaven, G. M. (1988). Banting lecture 1988. Role of insulin resistance in human disease. Diabetes, 37(12), 1595-1607.
- 간략한 내용: ‘대사증후군’이라는 용어가 대중화되기 전, 스탠포드 대학교의 제럴드 리븐(Gerald Reaven) 박사가 1988년 당뇨병학회에서 발표한 밴팅 강연 논문입니다. 이 강연에서 그는 인슐린 저항성이 제2형 당뇨병뿐만 아니라 고혈압, 고중성지방혈증, 낮은 HDL 콜레스테롤, 관상동맥 질환 등 다양한 질환의 공통적인 원인임을 강력하게 주장하며 **”신드롬 X (Syndrome X)”**라는 개념을 제시했습니다. 이 논문은 인슐린 저항성이 여러 만성 질환의 연결 고리임을 명확히 한 기념비적인 연구로 평가받습니다.
- DeFronzo, R. A., & Ferrannini, E. (1991). Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Advances in Internal Medicine, 36, 237-279.
- 간략한 내용: 리븐 박사의 개념을 확장하여 인슐린 저항성이 비인슐린의존성 당뇨병(NIDDM, 현재의 제2형 당뇨병), 비만, 고혈압, 이상지질혈증 및 죽상경화증을 포함하는 복합적인 증후군이라는 점을 심층적으로 다룬 리뷰 논문입니다. 인슐린 저항성이 어떻게 이러한 질환들을 일으키는 복잡한 생리학적 메커니즘을 유발하는지 상세히 설명합니다.
- Lustig, R. H. (2012). Fructose 2.0: The elephant in the kitchen. Obesity, 20(3), 481-482.
- 간략한 내용: 설탕, 특히 과당(Fructose),액상과당(HFCS) 섭취가 비만, 인슐린 저항성 및 대사 질환에 미치는 영향에 대한 논의를 촉발시킨 대표적인 논문 중 하나입니다. 소아 내분비학자인 로버트 러스티그(Robert H. Lustig)는 과당이 간에서 대사되는 방식이 인슐린 저항성과 지방간 형성에 어떻게 기여하는지 강조하며, 단순 칼로리 섭취를 넘어 영양소의 질과 종류가 중요함을 역설합니다. 그의 저서 **《The Hacking of the American Mind》**나 **《Fat Chance》**에서도 이러한 관점을 더 자세히 다루고 있습니다.
- Fung, J. (2016). The Obesity Code: Unlocking the Secrets of Weight Loss. Greystone Books.
- 간략한 내용: 신장내과 의사인 제이슨 펑(Jason Fung) 박사의 베스트셀러 저서입니다. 이 책은 비만을 단순한 칼로리 섭취량의 문제가 아닌, 호르몬, 특히 인슐린 수치의 문제로 접근하며 인슐린 저항성과 고인슐린혈증이 비만과 대사 질환의 핵심 원인임을 강조합니다. 간헐적 단식과 저탄수화물 식단이 인슐린 수치를 낮춰 인슐린 저항성을 개선하고 체중 감량에 기여하는 메커니즘을 대중적인 언어로 설명하며 큰 영향을 미쳤습니다.
Metabolic Health and Insulin Resistance: A Major Health Challenge for Modern People
In the last part, we looked at insulin, the first peptide drug in human history and also the first drug developed using genetic engineering. This time, we’ll delve into the insulin hormone naturally secreted by our bodies and explore the concept of insulin resistance.
Metabolic Syndrome: A Closer Threat Than We Think
According to recently released 2024 data, roughly half (47.0%) of adults aged 65 and over in South Korea are experiencing metabolic syndrome. This isn’t just a Korean problem; metabolic health issues are severe worldwide, and their prevalence is increasing with an aging global population.
When we talk about metabolic syndrome, we often focus on individual metrics like blood pressure, blood sugar, triglycerides, cholesterol, and abdominal fat. However, metabolic syndrome, where all these indicators are intricately intertwined, goes beyond being a simple sum of individual numbers. What common underlying cause connects these diverse symptoms that appear together?
Insulin Resistance: The Key to Metabolic Problems
Since the early 20th century, particularly with research accelerating after the 1960s, modern medicine has identified insulin resistance as one of the fundamental causes of metabolic syndrome and numerous chronic diseases.
Medical professionals sometimes explain insulin resistance simply as “a state where our body’s cells don’t respond normally to the hormone insulin, leading the pancreas to over-secrete insulin, resulting in hyperinsulinemia.” But sometimes, overly condensed information can fail to convey the full picture. It’s important to delve deeper into the meaning of insulin resistance and its mechanisms.
Understanding Insulin Resistance and Its Mechanisms
Insulin doesn’t just “guide” glucose into cells; it acts as a signaling molecule that “instructs” cells to effectively absorb and utilize glucose.
- Insulin’s Target Tissues and Receptors: For insulin to act on specific cells, those cells must have insulin receptors on their surface. When insulin binds to these receptors, a series of signals is transmitted inside the cell. These signals cause glucose transporters to move to the cell membrane, opening pathways for glucose to enter the cell. Insulin resistance means that there’s a problem with these receptors or the subsequent signaling process, causing the cells to become less sensitive to insulin’s instructions.
- Organs Without Glucose Requirement: Some organs in our body (e.g., parts of the brain, red blood cells) have specific glucose receptors (like GLUT1, GLUT3) that allow them to absorb glucose without insulin’s help. These organs aren’t directly affected by insulin resistance. However, the primary targets of insulin resistance are the liver, skeletal muscle, and adipose (fat) tissue. When insulin resistance develops in these tissues, it leads to significant problems with systemic blood sugar control.
Insulin’s Role in Fat Metabolism: More Than Just Blood Sugar
Insulin is deeply involved not only in glucose metabolism but also in fat metabolism.
- Promoting Fat Accumulation: Insulin plays a crucial role in promoting fatty acid synthesis in the liver and fat tissue, and in stimulating fat cells to absorb glucose, converting it into triglycerides for storage.
- Inhibiting Fat Breakdown: It also inhibits the breakdown of fat in fat cells. This means insulin is a very important hormone for our body to store energy and accumulate fat.
When Insulin Resistance Occurs: If insulin resistance develops, problems also arise in these fat metabolism regulatory functions. When fat cells become insensitive to insulin signals, blood fatty acid levels rise. This, in turn, can lead to fatty liver disease or abnormal fat accumulation in other tissues (ectopic fat). This ectopic fat then creates a vicious cycle, further worsening insulin resistance.
Thus, insulin resistance isn’t just a blood sugar control issue; it causes complex dysfunctions across both glucose and fat metabolism. This ultimately contributes to metabolic syndrome, type 2 diabetes, cardiovascular disease, and even certain types of cancer (such as breast and pancreatic cancer).
Research findings, including those by Reaven (1988) and DeFronzo & Ferrannini (1991), demonstrate that hyperinsulinemia is a key mechanism driving various symptoms of metabolic dysfunction and metabolic syndrome. And the most fundamental cause of this hyperinsulinemia stems from chronic overconsumption of glucose or digestible carbohydrates that can be easily converted into glucose from our food.
References
Our understanding of insulin resistance has evolved through decades of extensive research. The following are key milestones in this field.
- Himsworth, H. P. (1939). Diabetes Mellitus: Its Differentiation into Insulin-Sensitive and Insulin-Insensitive Types. The Lancet, 233(6022), 127-130.
- Brief Description: This significant paper, published not long after the discovery of insulin (1921), shows early attempts to differentiate diabetes into insulin-sensitive and insulin-insensitive types. This can be seen as a cornerstone of the modern concept of ‘insulin resistance,’ offering insights that differences in insulin responsiveness might underlie the disease.
- Reaven, G. M. (1988). Banting lecture 1988. Role of insulin resistance in human disease. Diabetes, 37(12), 1595-1607.
- Brief Description: This is a landmark lecture by Dr. Gerald Reaven of Stanford University, presented at the American Diabetes Association in 1988, predating the popularization of the term ‘metabolic syndrome.’ In this lecture, he strongly argued that insulin resistance is a common underlying cause of not only type 2 diabetes but also hypertension, hypertriglyceridemia, low HDL cholesterol, and coronary artery disease, proposing the concept of “Syndrome X.” This paper is considered pivotal for clearly establishing insulin resistance as the link between various chronic diseases.
- DeFronzo, R. A., & Ferrannini, E. (1991). Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Advances in Internal Medicine, 36, 237-279.
- Brief Description: Expanding on Dr. Reaven’s concept, this review article extensively covers insulin resistance as a multifaceted syndrome responsible for non-insulin-dependent diabetes mellitus (NIDDM, now type 2 diabetes), obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. It details the complex physiological mechanisms by which insulin resistance leads to these conditions.
- Lustig, R. H. (2012). Fructose 2.0: The elephant in the kitchen. Obesity, 20(3), 481-482.
- Brief Description: This is one of the seminal papers that ignited the discussion about the impact of sugar, especially fructose(HFCS), on obesity, insulin resistance, and metabolic diseases. Robert H. Lustig, a pediatric endocrinologist, emphasizes how the liver’s metabolism of fructose contributes to insulin resistance and fatty liver formation, stressing the importance of nutrient quality and type beyond simple caloric intake. His books, such as 《The Hacking of the American Mind》 and 《Fat Chance》, delve into these perspectives in more detail.
- Fung, J. (2016). The Obesity Code: Unlocking the Secrets of Weight Loss. Greystone Books.
- Brief Description: This bestselling book by nephrologist Dr. Jason Fung approaches obesity not merely as a matter of calorie intake, but as a hormonal issue, particularly concerning insulin levels. It highlights insulin resistance and hyperinsulinemia as the core causes of obesity and metabolic diseases. The book explains the mechanisms by which intermittent fasting and low-carbohydrate diets lower insulin levels, improve insulin resistance, and contribute to weight loss in accessible language, having a significant impact.
代謝の健康とインスリン抵抗性:現代人の主要な健康課題
前回の記事では、人類初のペプチド薬であり、遺伝子技術を応用した初の医薬品であるインスリンについて考察しました。今回は、私たちの体内で自然に分泌される重要なホルモン、インスリン、そしてインスリン抵抗性という概念について深く掘り下げて考えていきます。
メタボリックシンドローム:私たちが思うよりも身近な脅威
最近発表された2024年のデータによると、韓国では65歳以上の成人のおよそ半数(47.0%)がメタボリックシンドロームを患っているとされています。これは決して韓国だけの問題ではありません。世界的に代謝の健康問題は深刻であり、高齢化とともにその有病率はさらに上昇しています。
私たちはメタボリックシンドロームについて話すとき、血圧、血糖、中性脂肪、コレステロール、腹部脂肪といった個々の数値に注目しがちです。しかし、これらすべての指標が複雑に絡み合って現れるメタボリックシンドロームは、単なる個々の数値の合計を超えたものです。このように多様な症状が複合的に現れる背景には、どのような共通の原因が隠されているのでしょうか?
インスリン抵抗性:代謝問題の核心を握る鍵
現代医学は20世紀初頭から、特に1960年代以降に活発に進められた研究の結果、メタボリックシンドロームと多数の慢性疾患の根本的な原因の一つとして、インスリン抵抗性を指摘してきました。
医療専門家は、インスリン抵抗性を「私たちの体の細胞がホルモンであるインスリンに正常に反応できない状態であり、その結果、膵臓が過剰にインスリンを分泌し、高インスリン血症が発生する」と簡潔に説明することもあります。しかし、時にはあまりに圧縮された情報が、かえって核心を伝えきれないこともあります。インスリン抵抗性の意味とそのメカニズムについて、もう少し具体的に掘り下げて考える必要があります。
インスリン抵抗性とそのメカニズム
インスリンは、単にブドウ糖を細胞へ「案内」する役割だけではありません。インスリンは、細胞がブドウ糖を効果的に吸収し利用できるように「指示」するシグナル伝達物質としての役割を果たしています。
- インスリンの標的組織と受容体: インスリンが特定の細胞に作用するためには、その細胞表面にインスリン受容体が存在している必要があります。インスリンがこの受容体に結合すると、細胞内部に一連のシグナルが伝達され、このシグナルによってブドウ糖輸送体が細胞膜に移動し、ブドウ糖が細胞内に入るための通路を開きます。インスリン抵抗性とは、まさにこの受容体とそれ以降のシグナル伝達過程に問題が生じ、細胞がインスリンの指示に鈍感になることを意味します。
- ブドウ糖が不要な臓器: 私たちの体の一部の臓器(例:脳の一部、赤血球)は、インスリンの助けなしにブドウ糖を吸収できる特定のブドウ糖受容体(GLUT1、GLUT3など)を持っています。これらの臓器はインスリン抵抗性の直接的な影響を受けません。しかし、インスリン抵抗性の主な標的は肝臓、骨格筋、脂肪組織であり、これらの組織でインスリン抵抗性が発生すると、全身の血糖調節に深刻な問題が生じます。
インスリンの脂肪代謝への関与:単なる血糖問題ではない
インスリンはブドウ糖代謝だけでなく、脂肪代謝にも深く関与しています。
- 脂肪蓄積の促進: インスリンは肝臓や脂肪組織で脂肪酸合成を促進し、脂肪細胞へブドウ糖を吸収させて中性脂肪に変換し、貯蔵する重要な役割を果たします。
- 脂肪分解の抑制: また、脂肪細胞での脂肪分解を抑制します。つまり、インスリンは私たちの体がエネルギーを貯蔵し、脂肪を蓄積する上で非常に重要なホルモンなのです。
インスリン抵抗性発生時: インスリン抵抗性が発生すると、これらの脂肪代謝調節機能にも問題が生じます。脂肪細胞がインスリンシグナルに鈍感になると、血中の脂肪酸レベルが上昇し、これは再び肝臓へ向かい脂肪肝を引き起こしたり、他の組織に異常な脂肪が蓄積する**異所性脂肪(Ectopic Fat)**を招いたりします。そしてこの異所性脂肪が、さらにインスリン抵抗性を悪化させる悪循環を生み出します。
このように、インスリン抵抗性は単なる血糖調節の問題にとどまらず、ブドウ糖と脂肪代謝全般にわたる複合的な異常を引き起こし、それが結果的にメタボリックシンドローム、2型糖尿病、心血管疾患、さらには特定の種類のがん(乳がん、膵臓がんなど)の原因となり得ます。
Reaven(1988)やDeFronzo & Ferrannini(1991)をはじめとする複数の研究結果は、高インスリン血症が代謝異常とメタボリックシンドロームの多様な症状を引き起こす核心的なメカニズムであることを示しています。そして、この高インスリン血症の最も根本的な原因は、食事から摂取するブドウ糖、あるいはブドウ糖に容易に変換される消化性の炭水化物の慢性的な過剰摂取に起因します。
参考文献
インスリン抵抗性に関する理解は、数十年にわたる広範な研究を通じて発展してきました。以下は、この分野の主要な節目となった文献です。
- Himsworth, H. P. (1939). Diabetes Mellitus: Its Differentiation into Insulin-Sensitive and Insulin-Insensitive Types. The Lancet, 233(6022), 127-130.
- 概要: インスリンが発見されて間もない時期(1921年)に、すでに糖尿病をインスリン感受性型とインスリン不感受性型に分類しようとする初期の試みを示した重要な論文です。これは現代の「インスリン抵抗性」概念の基礎を築いたと言え、インスリンに対する反応性の違いが疾患の根底にある可能性を示唆しています。
- Reaven, G. M. (1988). Banting lecture 1988. Role of insulin resistance in human disease. Diabetes, 37(12), 1595-1607.
- 概要: 「メタボリックシンドローム」という用語が一般化する以前の1988年、スタンフォード大学のジェラルド・リーベン博士が糖尿病学会で発表したバンティング講演論文です。この講演で彼は、インスリン抵抗性が2型糖尿病だけでなく、高血圧、高トリグリセリド血症、低HDLコレステロール、冠動脈疾患など、多様な疾患の共通原因であると強く主張し、**「シンドロームX(Syndrome X)」**という概念を提唱しました。この論文は、インスリン抵抗性が様々な慢性疾患のつながりであることを明確にした画期的な研究として評価されています。
- DeFronzo, R. A., & Ferrannini, E. (1991). Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Advances in Internal Medicine, 36, 237-279.
- 概要: リーベン博士の概念を拡張し、インスリン抵抗性が非インスリン依存性糖尿病(NIDDM、現在の2型糖尿病)、肥満、高血圧、脂質異常症、アテローム性動脈硬化性心血管疾患を含む多面的な症候群であるという点を深く掘り下げた総説論文です。インスリン抵抗性がこれらの疾患を引き起こす複雑な生理学的メカニズムを詳細に解説しています。
- Lustig, R. H. (2012). Fructose 2.0: The elephant in the kitchen. Obesity, 20(3), 481-482.
- 概要: 砂糖、特に果糖の摂取が肥満、インスリン抵抗性、および代謝性疾患に与える影響についての議論を巻き起こした代表的な論文の一つです。小児内分泌学者であるロバート・ラスティグ氏は、果糖,HFCSが肝臓で代謝される方法がインスリン抵抗性や脂肪肝の形成にどのように寄与するかを強調し、単なるカロリー摂取量を超えて栄養素の質と種類が重要であることを力説しています。彼の著書**『The Hacking of the American Mind』や『Fat Chance』**でも、これらの視点がより詳細に語られています。
- Fung, J. (2016). The Obesity Code: Unlocking the Secrets of Weight Loss. Greystone Books.
- 概要: 腎臓専門医であるジェイソン・ファン博士のベストセラー著書です。この本は肥満を単なるカロリー摂取量の問題ではなく、ホルモン、特にインスリンレベルの問題として捉え、インスリン抵抗性と高インスリン血症が肥満と代謝性疾患の核心的な原因であることを強調しています。間欠的断食と低炭水化物ダイエットがインスリンレベルを下げ、インスリン抵抗性を改善し、体重減少に貢献するメカニズムを一般読者にも分かりやすい言葉で解説し、大きな影響を与えました。
Leave a Reply